Pathophysiology of Lupus
Exact mechanism is not known. Alterations in the immune system and cellular antibodies such as antinuclear antibodies, deoxyribonucleuic acid (DNA), antihistones, and antibodies to ribonucleoprotein are strongly associated with SLE. There are abnormalities of both B and T cells in persons with the disease also. The increase of B cells are thought to cause an increase in the production of antibodies to self and non-self antigen. This is responsible for the tissue injury seen in SLE.
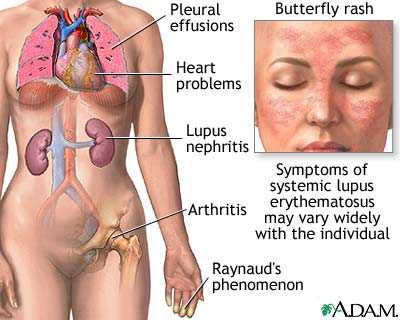
Clinical ManifestationsGeneral: fatigue, malaise. episodic fever
Musculoskeletal: arthralgia, arthritis, morning stiffness, joint deformities Skin: photo-sensitivity, butterfly rash, discoid lesions of skin and mucous membranes, alopecia, telangiectasia Neurologic: neuropathy, stroke, headache, seizures Pulmonary: cough, dyspnea, pleurisy, pneumonitis Gastrointestinal: dysphagia, nausea, vomiting, pancreatitis, elevated liver function test |
Cardiovascular: Pericardial effusion, myocarditis, coronary artery disease, valvular disease, thrombophlebitis, Raynaud's phenomenon, vasculitis Hematologic: anemia, leukopenia, thrombocytopenia, lymphadenopathy, splenomegaly, antibodies to clotting factors Renal: nephritis, glomerulonephritis, urinary tract infection |
|

|

|
